Our website uses cookies and other similar tools. We also analyze anonymized web traffic. You can choose your cookie preferences below. You may choose only necessary cookies, specific cookies or all cookies. Read more in our privacy policy
Home > All articles > Sweden’s TLV Updates Reimbursement Model for Rare Diseases
Sweden’s TLV Updates Reimbursement Model for Rare Diseases
Sweden has introduced a new reimbursement model for orphan drugs, likely to increase treatment options for rare diseases. At the same time, pharmaceutical companies are now expected to provide local evidence.
The first ISPOR Nordic Chapter Inspirational Meeting brought together Nordic experts in cost-effectiveness, reimbursement, and real-world evidence (RWE) on April 1. Held online, the event featured presentations on current topics from various countries.
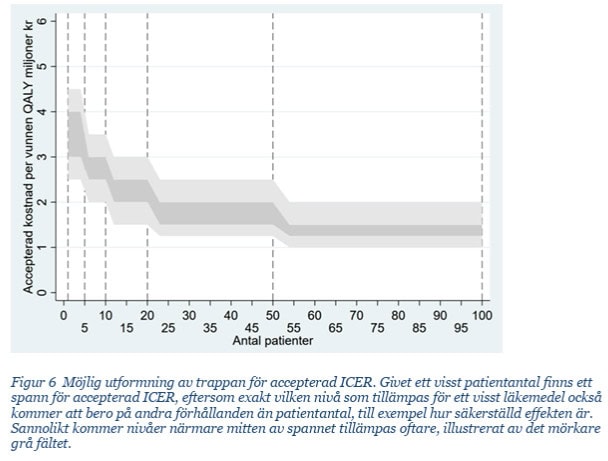
Under TLV’s new model, drugs intended for rare diseases may be granted a higher ICER threshold, referring to the cost per quality-adjusted life year (QALY). The ICER threshold reflects the level of cost-effectiveness society considers acceptable and how much it is willing to pay for different treatments. In the case of rare diseases, treatment options are typically limited, and drug development costs are high.
Challenges of Comprehensive Assessment
Under the TLV model, orphan drugs may receive higher reimbursement if they are intended for the treatment of serious conditions. TLV performs a holistic assessment of the drug’s cost-effectiveness, considering factors such as the impact of the disease on quality of life and the lack of treatment alternatives.
According to Hermansson, this comprehensive assessment introduces uncertainty for pharmaceutical companies and requires them to demonstrate benefits more precisely through data.
“If a company plans to bring a rare disease treatment to the Swedish market, it should start early in planning how to collect local data. High-quality data plays a key role in reimbursement decisions. Currently, companies typically rely on phase 3 data in their applications and often do not collect country-specific information in advance to support their evaluation process,” Hermansson emphasizes.
Sweden’s introduction of a higher ICER threshold specifically for rare diseases is unique in Nordic countries. Other Nordic authorities have not officially adopted similar models that raise the threshold based on rarity.
Finland’s New Regulation Facilitates Research on Rare Diseases
During the event, Findata shared updates on the potential for data utilization. As of early April, a new regulation allows Findata to provide cohorts as small as three patients—welcome news for rare disease research. Previously, the minimum cohort size available was five patients.
This change will make rare disease research in Finland more feasible, as small patient groups can now be better reflected in the data.
Lisse-Lotte started at Medaffcon 1st of October 2024. Previously she was at a Swedish-German company as CSO Chief Scientific Officer, consulting European companies about Nordic health data opportunities and market access. She has a M.Sc (Econ.) from Helsingin School of Economics and a M.Sc (Health Econ) from Karolinska. Additionally a Ph.D student at the University of Turku in Health Economics. She has obtained a long experience from global pharma and medtech. She has lived over 20 years in Sweden.
The current development gives new possibilities to utilise data. With AI we can produce synthetic data and build digital twins that can actually support drug development and support healthcare providers. Innovative solutions are only useful if they are adopted to daily practice.
Old ways of working will vanish and RWD will be acknowledged as an excellent option or support for RCTs. As RWD is enabling more cost-effective evidence generation for new treatments. Treatments need to be more personalised so that the right drugs, diagnostics and devices are used for the right patients at the right time.